
This case stresses the different varieties of presentation of placentomegaly , IUGR and doppler studies. Kindly go through last week’s case to appreciate the differences.
This was a 23 year old lady with h/o gravida 2 , para 0 , live , abortion 1 .
She came for a scan around 29 to 30 weeks of gestation . She had pregnancy induced hypertension detected 1 week ago .She had no history of hypertension during the earlier pregnancy , when the fetal loss had occurred after 3 months.
Her earlier scan done elsewhere 2 months before was reported as normal .
She had a thick placenta , but appears homogenous.

Biometric measurements show AC <2.3 %TILE



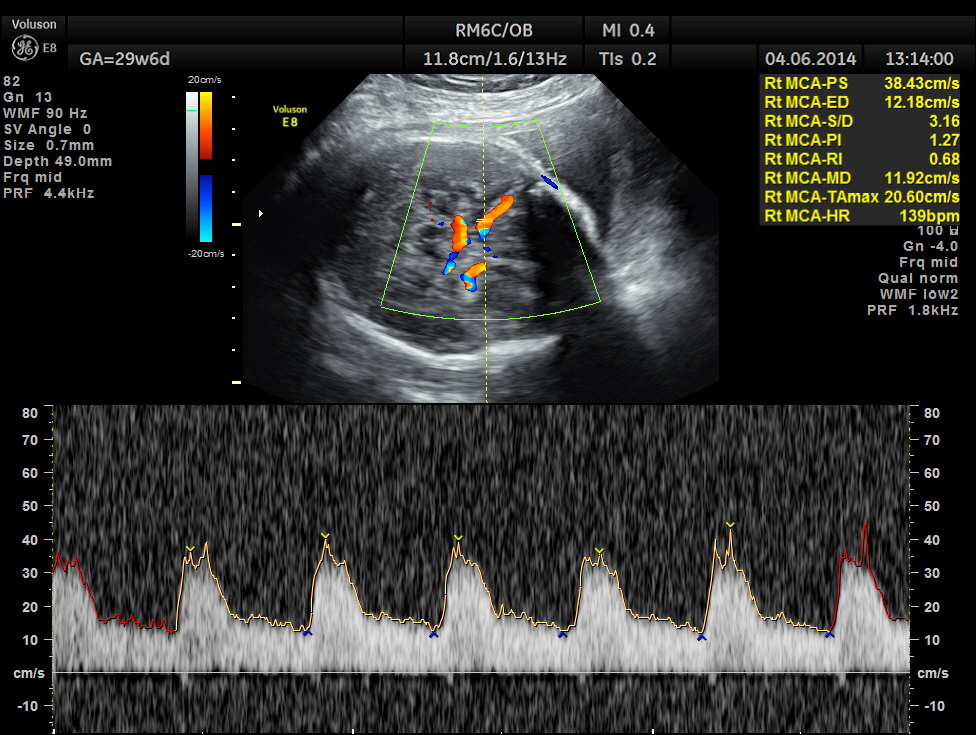
Umbilical artery P.I and R.I are high . The MCA / UMBILICAL arterial ratio is abnormal.

AFI appeared to be normal.
a




BPD , HC <10 % tile and AC is < 2.3 % tile .
AFI is normal .
But the doppler values are abnormal. Umbilical artery P.I. and R.I are > 95 % tile . MCA P.I. and R.I are lower .
The cerebroplacental ratio ( MCA/UA ratio ) is abnormally low -0.70 suggestive of utero placental insufficiency.
This patient was referred by her obstetrician to an institution for further management.
The following references might be of help.
Pulsatility index of the middle cerebral artery in normal fetuses –
http://www.ncbi.nlm.nih.gov/pubmed/21213492
The MCA PI decreased as gestational age advanced from 1.97 (SD 0.48) at 20 weeks to 1.15 (SD 0.18) at 37 weeks.
Fetal middle cerebral to uterine artery pulsatility index ratios in normal and pre-eclamptic pregnancies.
http://www.ncbi.nlm.nih.gov/pubmed/17029308
Normal MCA/uterine artery PI ratios decreased with advancing gestational age. Redistribution of the fetal circulation indicated by a low MCA/uterine artery PI ratio was seen in 30% of the mild (n=15) and 46% of the severe (n=30) pre-eclamptic cases. There was a significant difference between those without and those with signs of brain-sparing, respectively, in mean birth weight (2456.0 vs. 1424.5 g), gestational age at delivery (35.6 vs. 31.3 weeks) and gestational age at the time of examination (34.9 vs. 30.9 weeks). Furthermore, there was a significantly higher rate of small-for-gestational-age (SGA) neonates (57.8% vs. 25.7%), preterm delivery (100% vs. 81.8%) and Cesarean section (90.7% vs. 66.7%) in cases with an MCA/uterine artery PI ratio below the 5th percentile.
Changes observed in Doppler studies of the fetal circulation in pregnancies complicated by pre-eclampsia or the delivery of a small-for-gestational-age baby. I. Cross-sectional analysis.

Though what you have mentioned is greek & latin -the details… since how many yrs you r a sonologist too Krish….????
LikeLike
27 years
LikeLike
27
LikeLike
With MCA Dopplers angle is very important and I think that the measurement was not performed properly.
LikeLike
The angle is important when we are calculating the PSV ; when we are calculating PI and RI the angle will not change the values. You can do a Doppler in your machine and then angle correct and see , the PI and RI will be the same. I am giving a web link for your kind perusal
Check out Pulsed wave spectral Doppler (PW) from Clinical Ultrasound on Inkling
Thanks for your comments
https://www.inkling.com/read/allan-clinical-ultrasound-3rd/chapter-3/pulsed-wave-spectral-doppler-pw
LikeLike
There are two basic rules for spectral Doppler investigation.
1
Obtain a good sonogram by aligning the Doppler beam so that there is a good (typically <60–70° depending on the investigation) beam/flow angle to obtain adequate Doppler shifts. This is done by moving the transducer so that there is an adequate beam/flow angle. For linear arrays, beam steering may be used. Alter the scale so that the sonogram is clearly displayed.
2
If measurements of velocity are required, alter the Doppler cursor angle correction so that it is aligned with the direction of flow. Without this correction, the velocity scale and measurements made from it are incorrect (unless the beam and flow direction are very closely aligned).
If velocities are not required then rule 2 is not appropriate and it may be sufficient to obtain a good sonogram and make qualitative assessment of flow or measurements of non-dimensional indices such as resistance/resistive index and pulsatility index for which angle correction is not required.
LikeLike
Quick question..when doing an umbilical artery Doppler , what exactly are you looking at to determine if it’s normal? The S/D ratio? What is within normal range? Thanks…
LikeLike
Thank you my friend for such valuable and insightful articles. I especially found the one on MCA/Uterine artery ratio invaluable. Your images are well taken. I would love to work with you at some future time.
LikeLike
good dialogues
LikeLike
So what was the outcome? Also, how did you follow this mom and fetus? Biophysicals, NST’s, Venous Doppler? If delivered, what pushed you over the edge or did labor ensue spontaneously? Again, outcome please.
LikeLike
Hi. I really appreciate your effort kriznan. please do send me about Gynae color doppler study
LikeLike
To monitor IUGR we should start early interventions e.g. folic acid for both parents before pregnancy.
LikeLike