A 20 year old lady , 2nd gravida with one live normal child and history of consanguinity was referred for 2nd opinion for suspected cardiac anomaly.
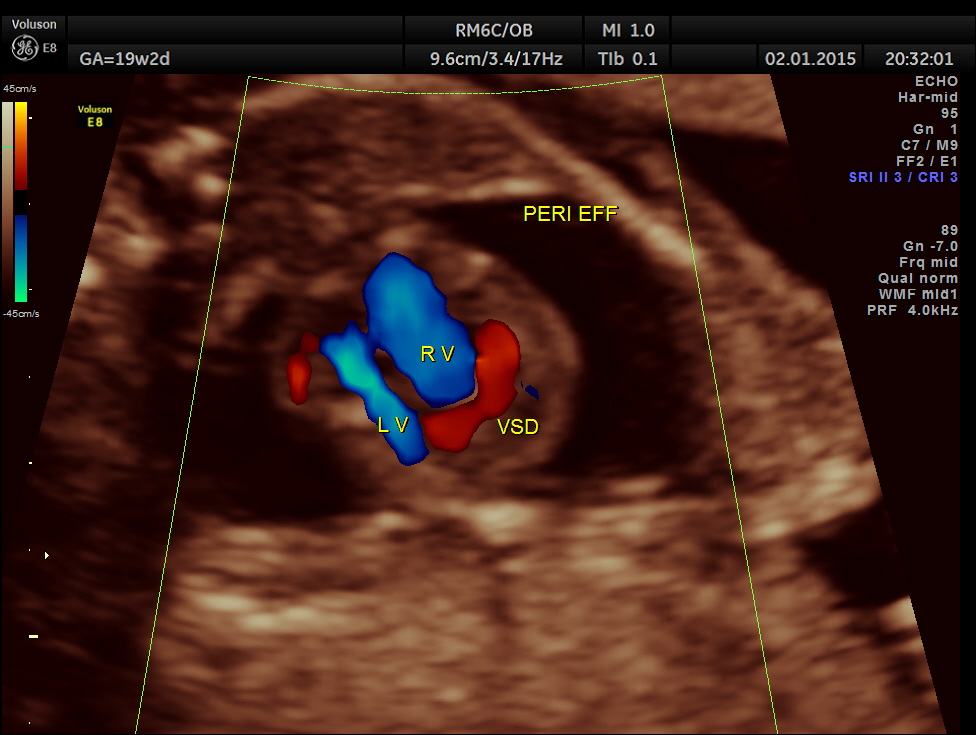
A large pericardial effusion is seen.


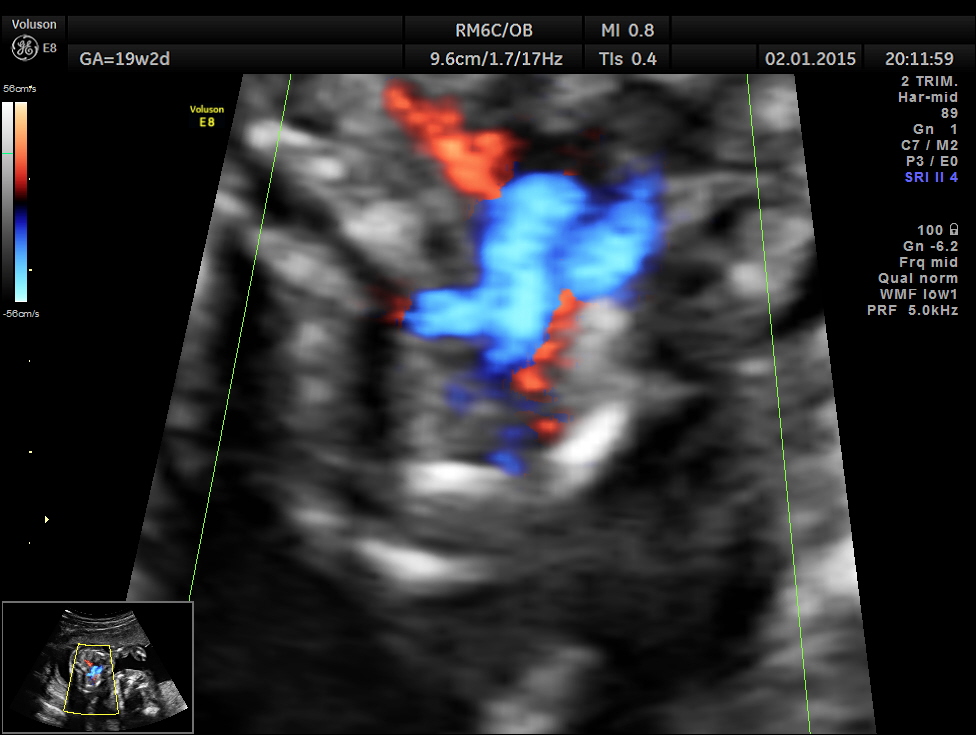
A prominent muscular ventricular septal defect is seen.

Apart from the VSD , left heart appears disproportionately smaller.


Great vessel crossing is seen.
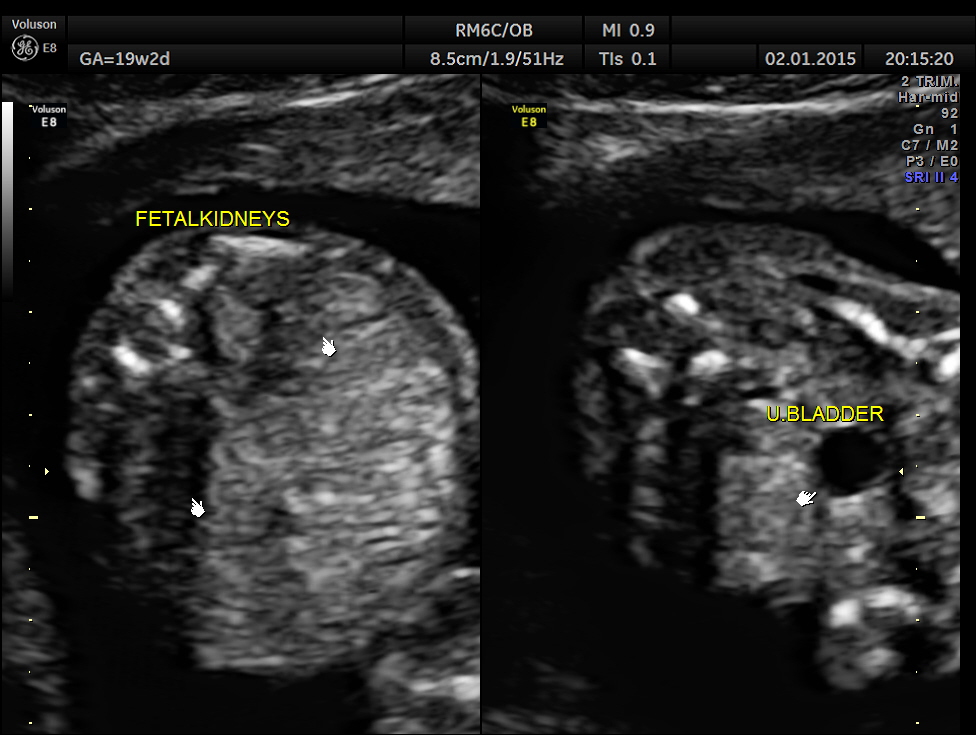

The rest of the scan findings were normal.




This fetus had a large pericardial effusion with structural defect of the heart – VSD and disproportionately smaller left heart – possibly co-arctation of aorta . The patient was advised chromosomal studies and was lost for follow up.
The following links give useful information .
http://radiopaedia.org/articles/fetal-pericardial-effusion
http://www.ncbi.nlm.nih.gov/pubmed/2660574
http://www.ncbi.nlm.nih.gov/pubmed/7932994
Click to access Cuneo-Pericardial-Effusion-3.pdf
http://www.visuog.com/Page/view.jsp?id=-1356523285267096104
The finding of a thin rim of pericardial fluid (< 2 mm) during routine prenatal ultrasound is not uncommon, being observed in more than 40-50% of normal fetuses , particularly when the ultrasound beam is perpendicular to the ventricular wall and pericardial surface. However, this has no clinical significance and is not considered as PE.
The incidence of true PE is unknown, since it should be considered as a marker of many other anomalies, eventually leading to fetal hydrops.
PE may be the result of the mechanism that produces non-immune fetal hydrops in a significant proportion of cases, thus presenting with other fluid collections (ascites, pleural effusion, skin edema). Structural cardiac malformations and arrhythmias are the most common cause, while other conditions associated with fetal hydrops include genetic disorders, metabolic disorders, tumors, hematologic abnormalities and congenital infections .
If the complete diagnostic work-up assessment is negative, the PE is classified as isolated. In such cases, the pathogenic mechanism is not well understood since most of the times the PE is transitory and regresses spontaneously .
PE may be a transitional finding in trisomy 21 fetuses, in the same fashion as increased nuchal translucency, thus their disappearance should not reassure in this regard. The risk of abnormal chromosomes is not related to the thickness of the effusion neither. Because of these data, fetal karyotyping should be discussed with parents, even in isolated pericardial effusion
Other causes could be
ventricular aneurysm or diverticulum
constriction of the ductus arteriosus,
idiopathic infantile arterial calcifications and cardiac tumors, mainly teratomas
PE is also associated with other congenital structural abnormalities such as diaphragmatic hernia/eventration , abdominal wall defects ,
and also with viral infections, including cytomegalovirus, Coxsackie A and B, parvovirus, human immunodeficiency virus and mycoplasma hominis .
PE has also been described to be associated with congenital hypothyroidism and maternal systemic lupus erythematosus , very likely related to a heart failure due to primary myocarditis or anemia.
