
This post has to be treated as part 2 of the last post – ASYMMETRY OF VENTRICLES – LV SMALLER THAN RV.
The following conditions should be thought of :
1. Co-arctation of Aorta
2. T.A.P.V.D. – Total Anomalous Pulmonary Venous Drainage ( or Connections )
3.Persistent Left Superior Vena Cava
4.Dilated Coronary Sinus
and rarely due to
5. Restricted Ductal Flow due to kinking of Ductus Arteriosus
6.Primary Myocardiopathy
7.Extra cardiac tumours
Most importantly this could be a normal fetus.
Out of these diagnosing Co-arctation of Aorta and T.A.P.V.D. antenatally could have major implications in prognosis.
Total Anomalous Pulmonary Venous Connections can have the following features. (ref :A Practical Guide to Fetal Echocardiography: Normal and Abnormal Hearts . By Alfred Z. Abuhamad, Rabih Chaoui )
TAPVC is a condition where all the pulmonary veins drain directly or indirectly into the right atrium.
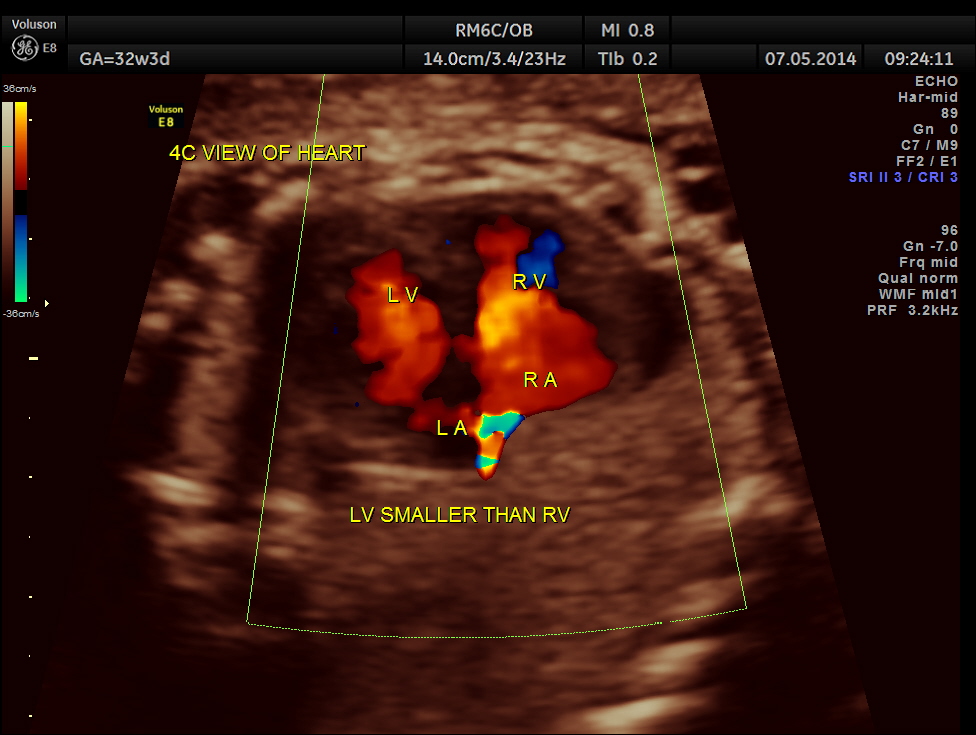
The 4 chamber view shows enlarged RA and RV and a confluence venous chamber behind the left atrium.
The 3 vessel trachea view shows a dilated Pulmonary artery and a vertical vein as the 4th vessel.
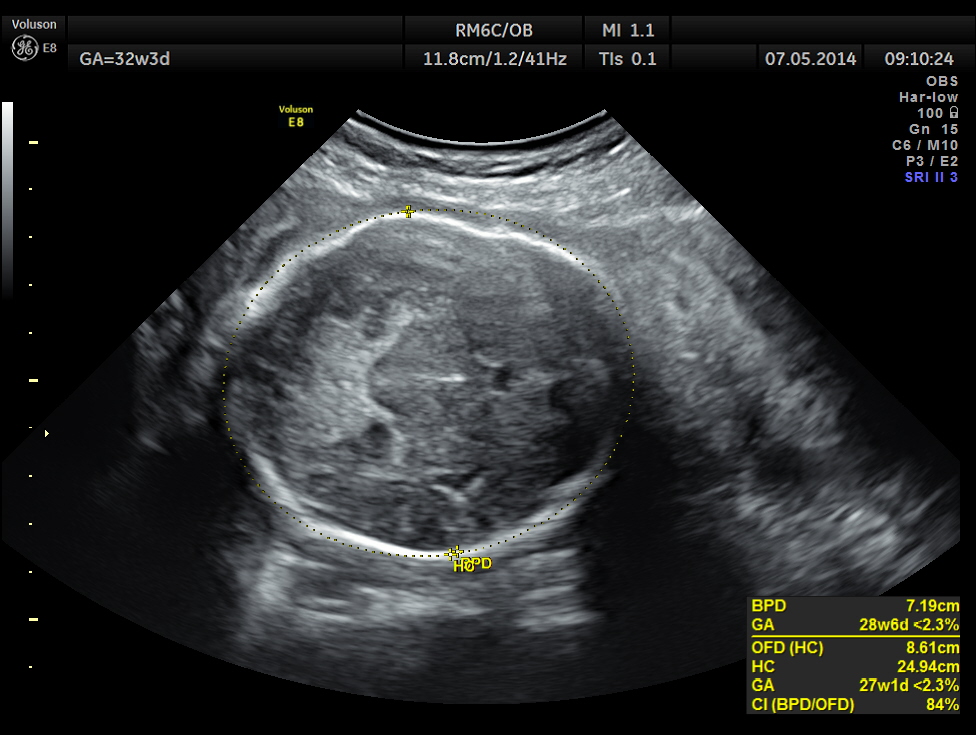
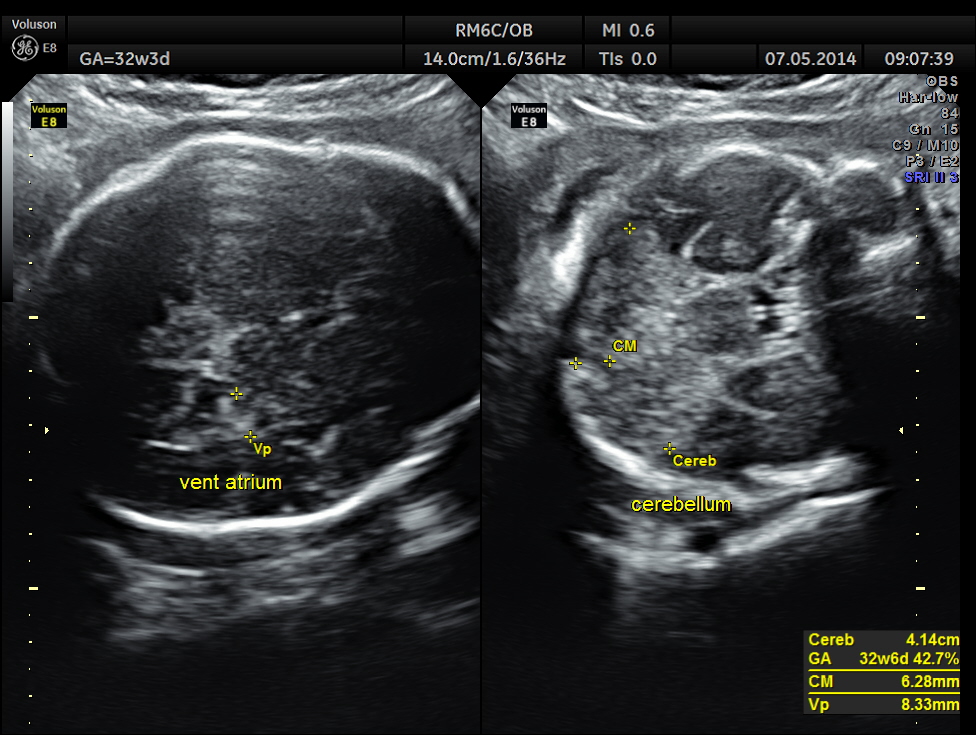
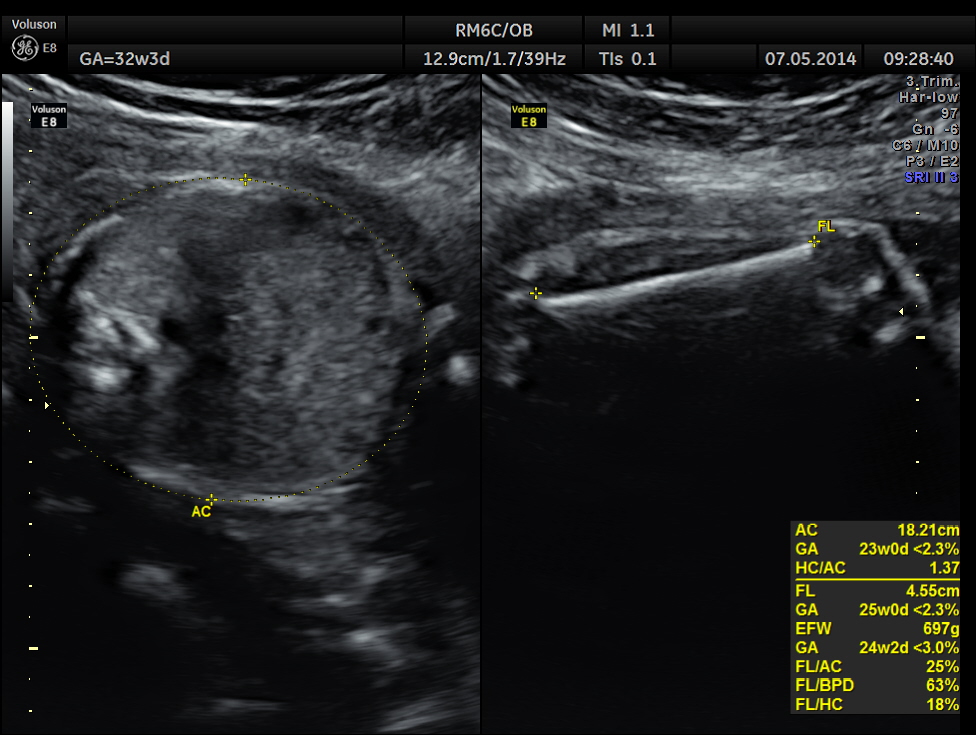
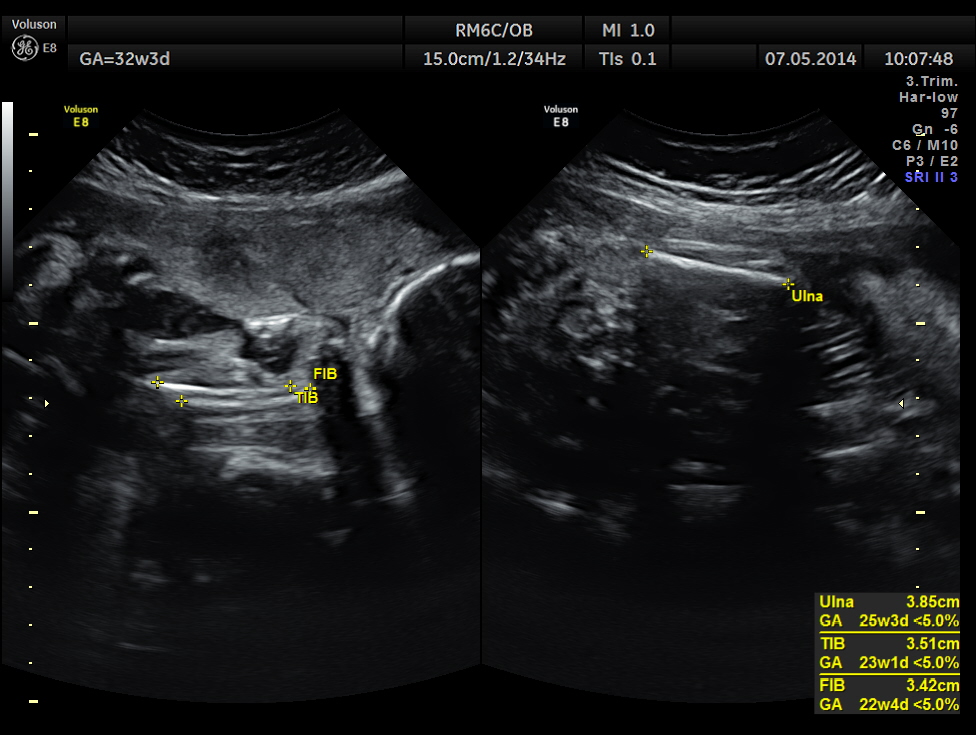
This was a 37 year old lady , a primi gravida referred for evaluation of intra uterine growth restriction. As per LMP the GA was 32 w 3 Days, but as per AUA the GA was 26 weeks . All the long bones were < 5.0 % tile. But cerebellum was 42.7 % tile. There was severe symmetrical growth restriction .
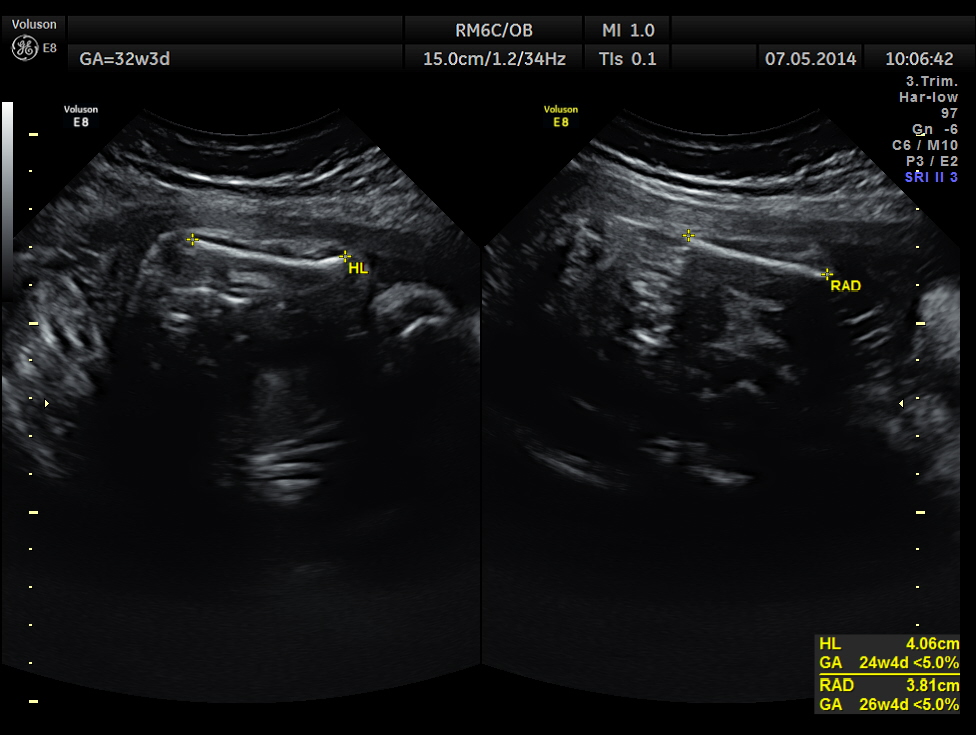
The echo pictures are given below.
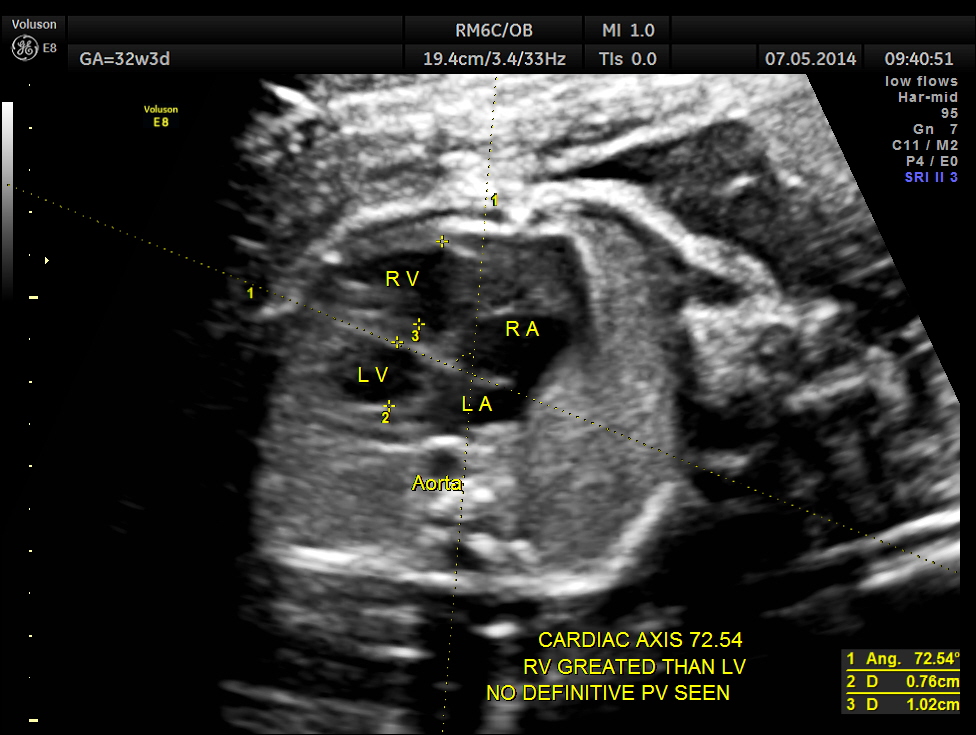
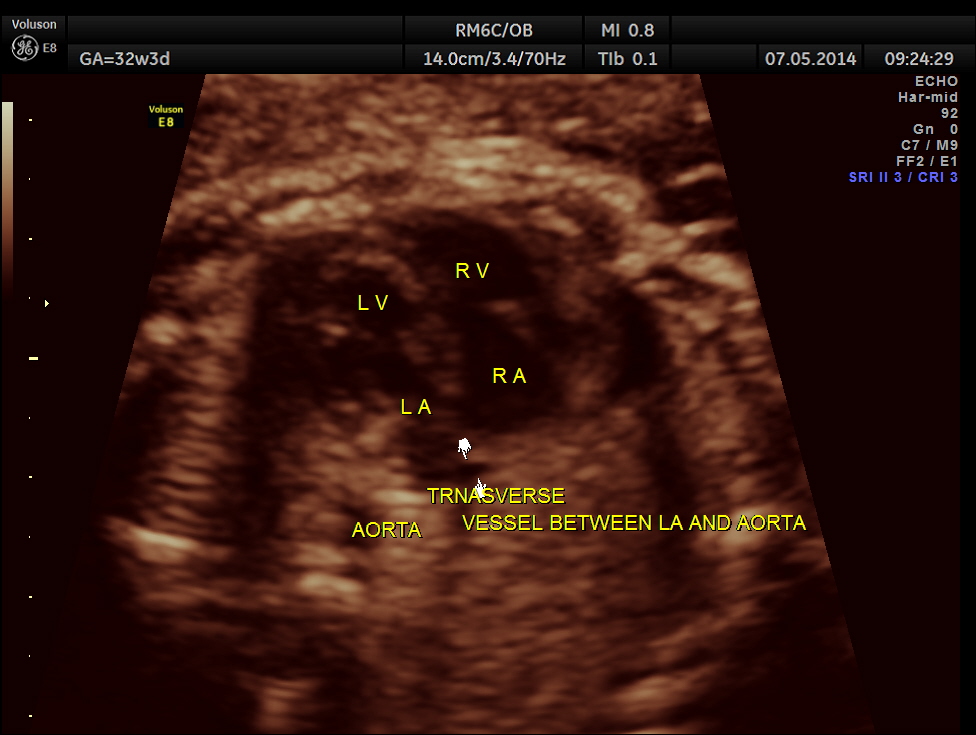
Cardiac axis is abnormal.
LA & LV appear to be smaller than RA & RV.
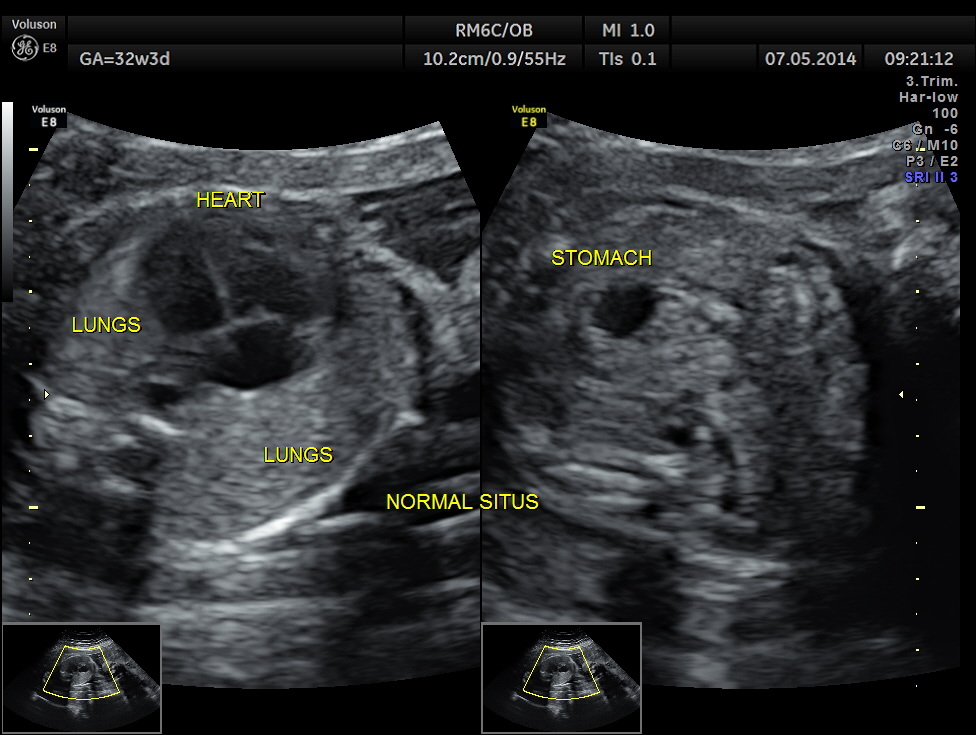
The situs appeared to be normal.
The following is a glass body imaging with a low flow setting. No pulmonary vein draining into LA could be made out.

The following picture is a glass body reconstruction showing the pulmonary vasculature.( given for comparison ).
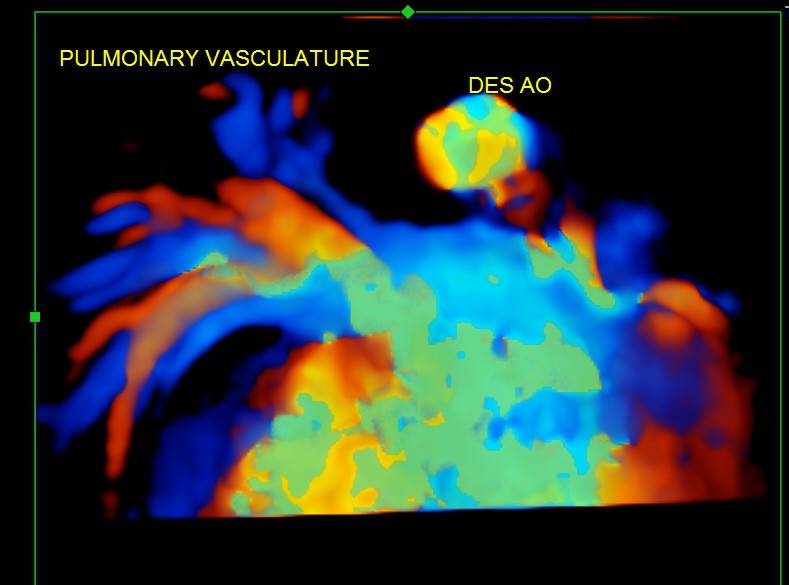
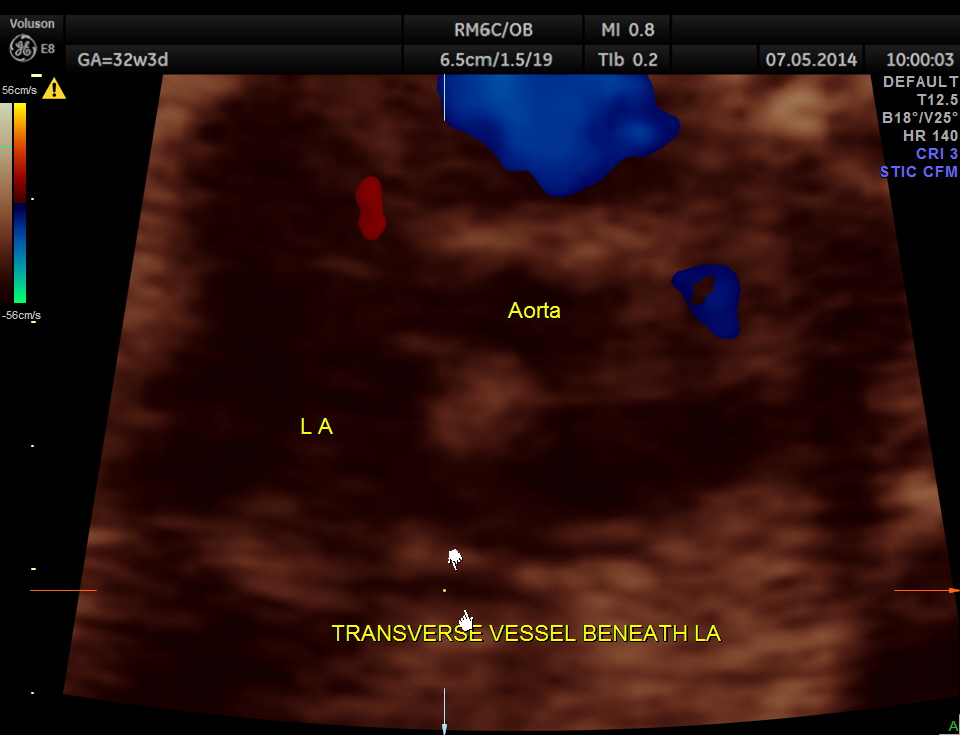
A transverse vessel is seen below the left atrium and is not seen to drain into the left atrium.
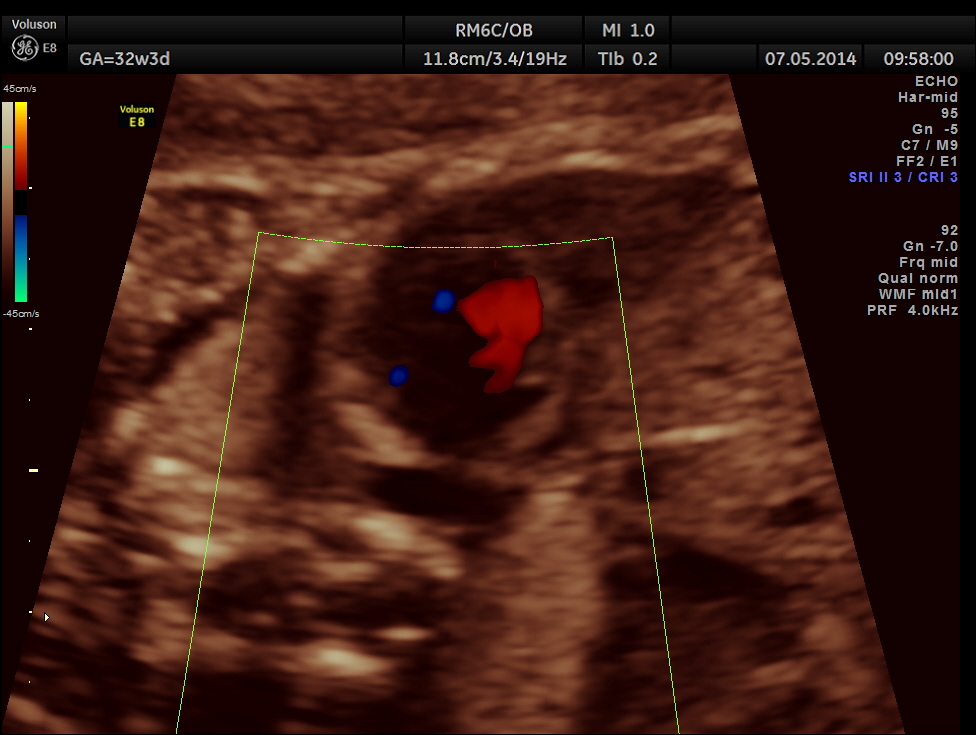
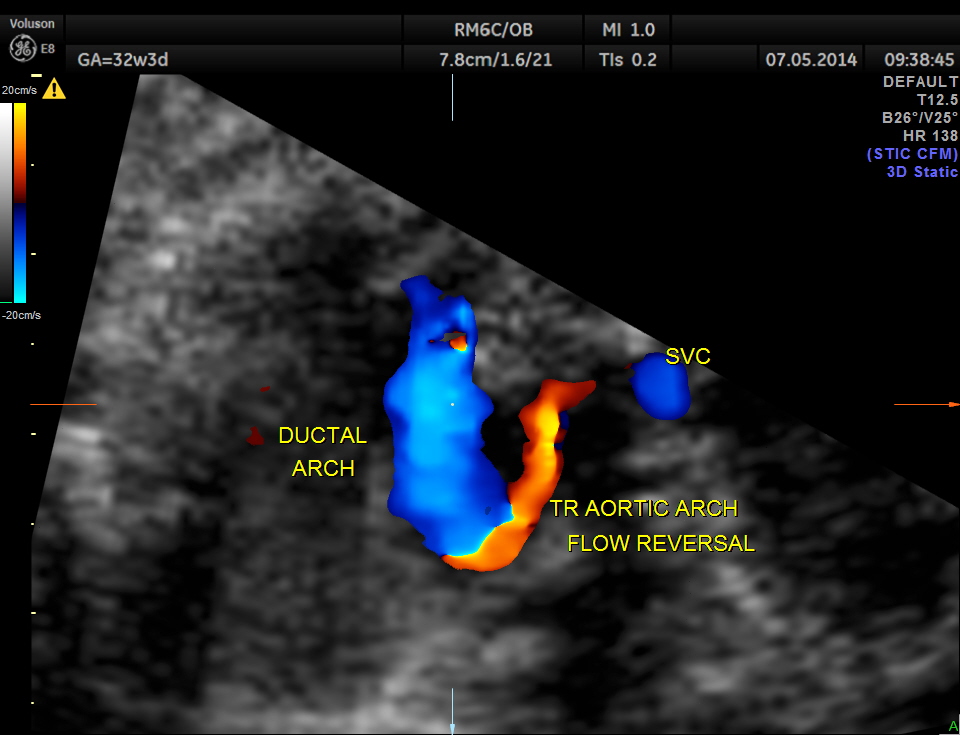
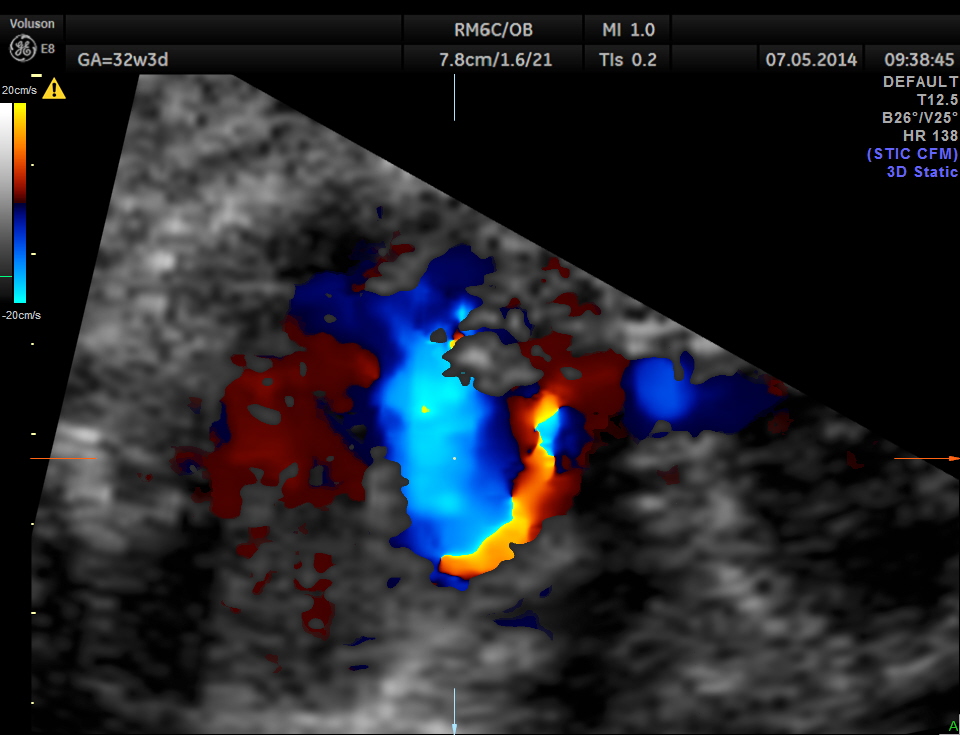
Ductal arch is prominently dilated in comparison to the aortic arch and there appears to be a flow reversal also.
3 vessel view also shows the pulmonary artery to be bigger in size than the aorta.
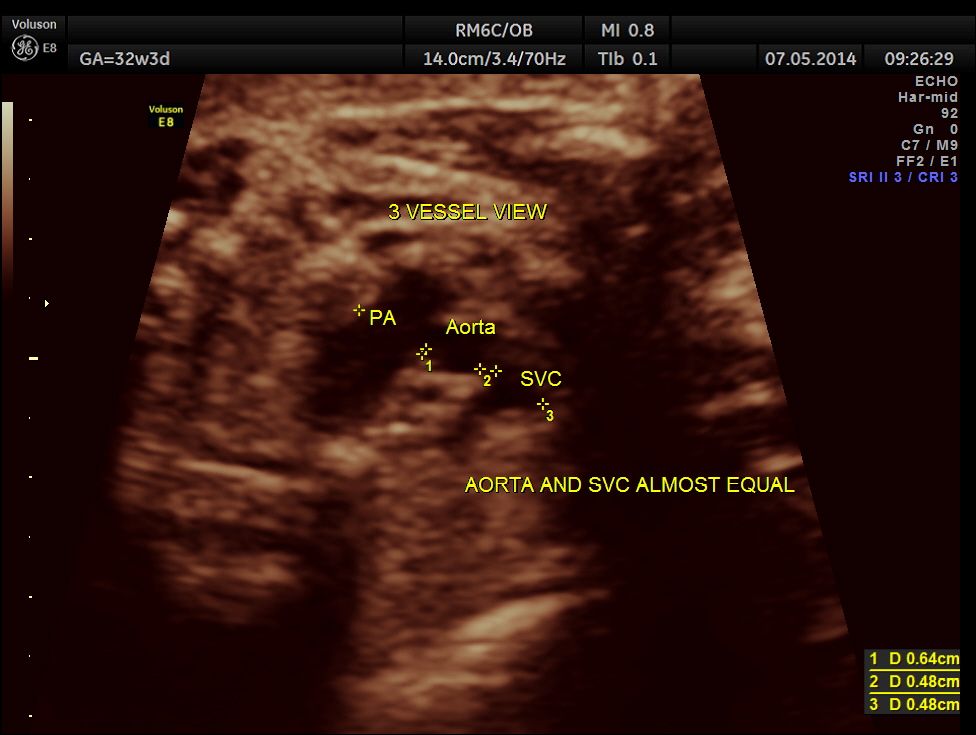
No definitive pulmonary vein draining into the left atrium could be made out . A common transverse vessel was seen beneath the left atrium . The LA & RA were smaller than the RA. Similarly the Aorta and the aortic arch were smaller than the pulmonary artery and the ductal arch due to the increased flow in the right side.
So a probable diagnosis of Total Anomalous Pulmonary Venous Connection with severe symmetric fetal growth restriction was offered. The patient apparently went into a spontaneous abortion and no autopsy study was done. So there is no confirmation again.
The following paper describes a new , novel way to detect TAPVC.
Post-LA space index” as a potential novel marker for the prenatal diagnosis of isolated total anomalous pulmonary venous connection

Thank you for the great case. I agree with your comments regarding the discrepancy in chamber sizes and the echo free space behind the LA in the presence of TAPVD. If this fetus has only TAPVD and no other co existing cardiac pathology, I don’t understand the great vessel discrepancy and would suspect an outflow obstructive lesion. I would also like to know if the IVC was intact.
Thanks for the great opportunity to participate
Jean Trines
LikeLike
Thanks for your comments.
LikeLike
Good case study!!
LikeLike
I enjoy your case presentations. Great images. Thank you.
Denise
LikeLike
Thank you
LikeLike
Hard work I like images
LikeLike