A 58 Year old lady presented to an emergency service of another hospital a day after Diwali festival with acute chest pain.
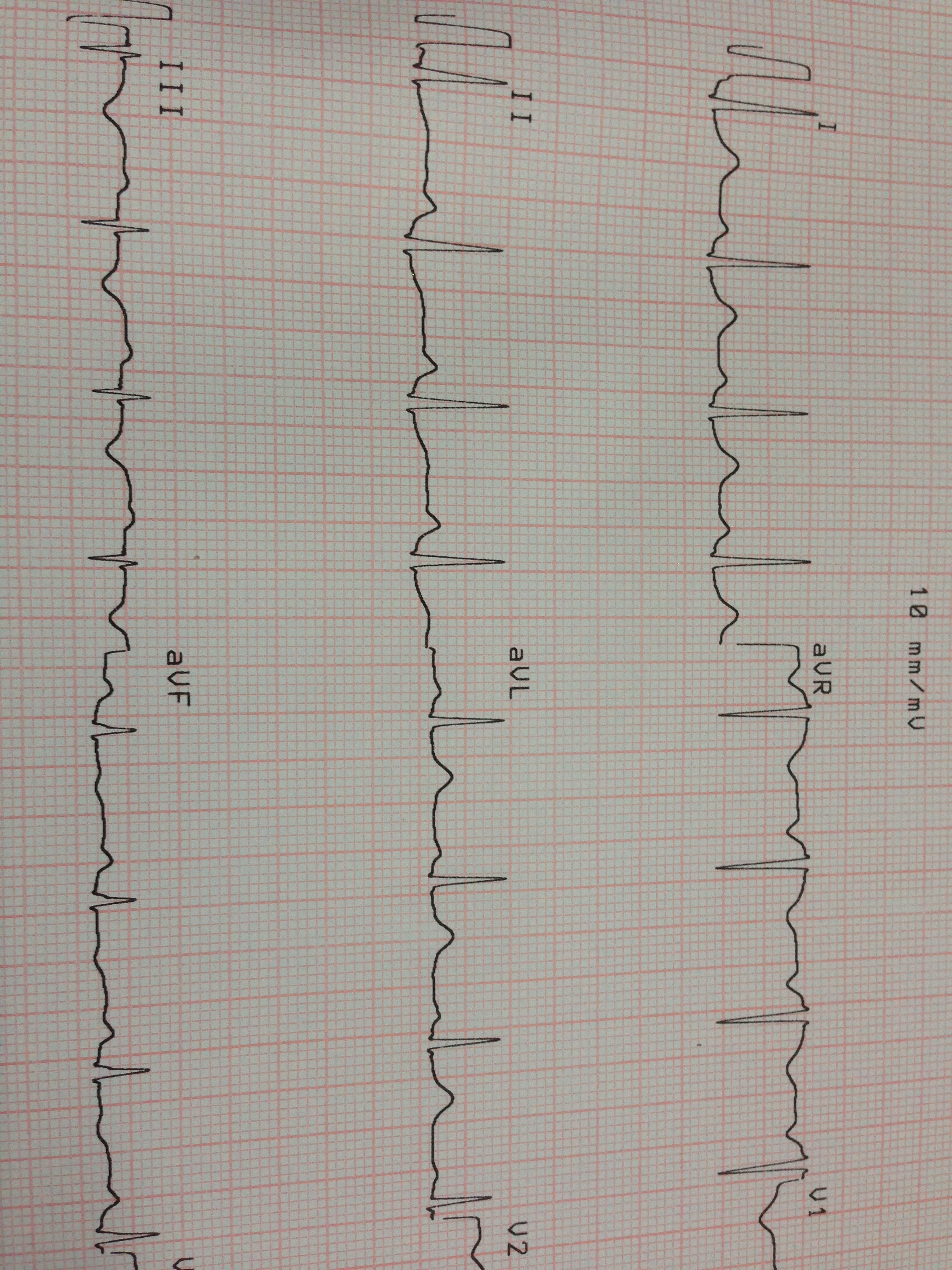
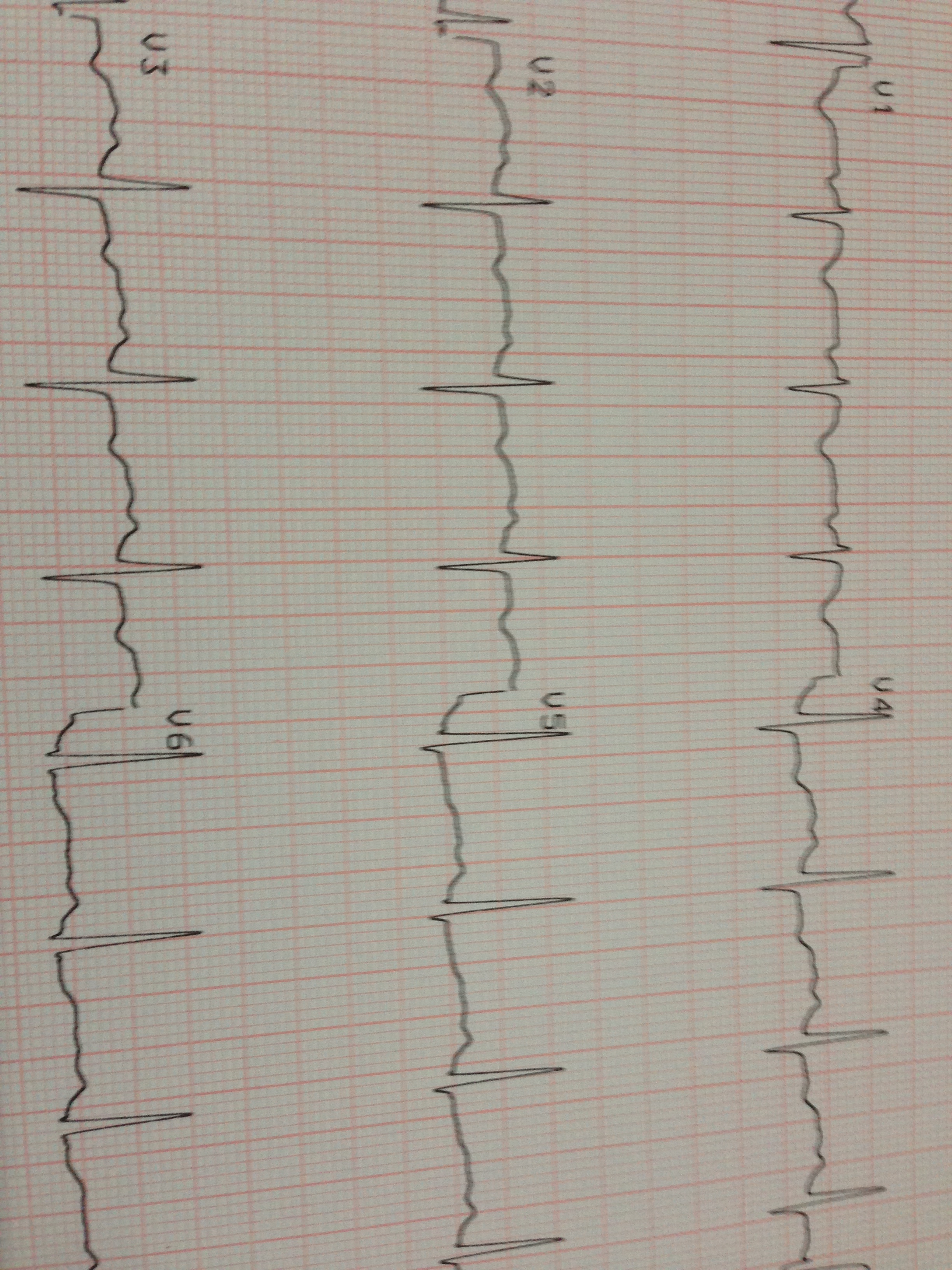
Her ECG showed T wave inversion in anterior and inferior wall leads. Her Troponin I was negative. Her ECHO was reported as normal. She was managed as an acute coronary syndrome in that hospital.
The ECG is given below.
She was discharged with partial relief of her pain with a prescription of high dose statin, clopidogrel , aspirin , anti anginals and PPI. . She was advised to report back if symptoms worsened for a coronary angiogram.
As she was not getting better , she went to a different cardiologist , who revised some of the anti anginals. She was still not getting better . Now she was having chest pain and vomiting and she came to me for consultation. The ECG showed similar changes. On examination she had tenderness over Murphy’s point.
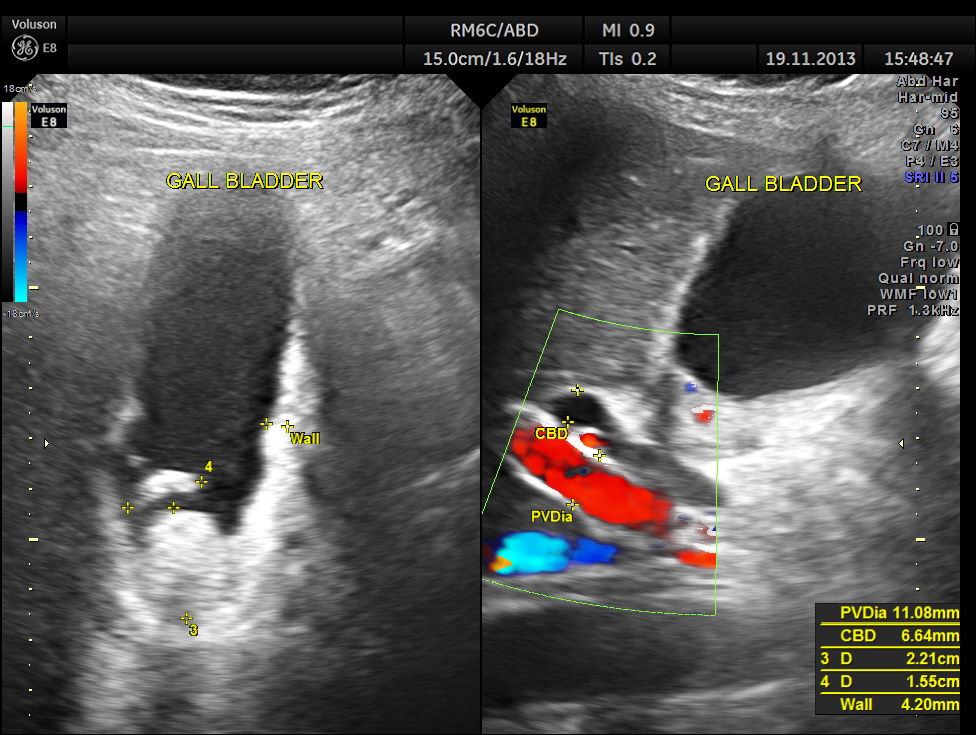
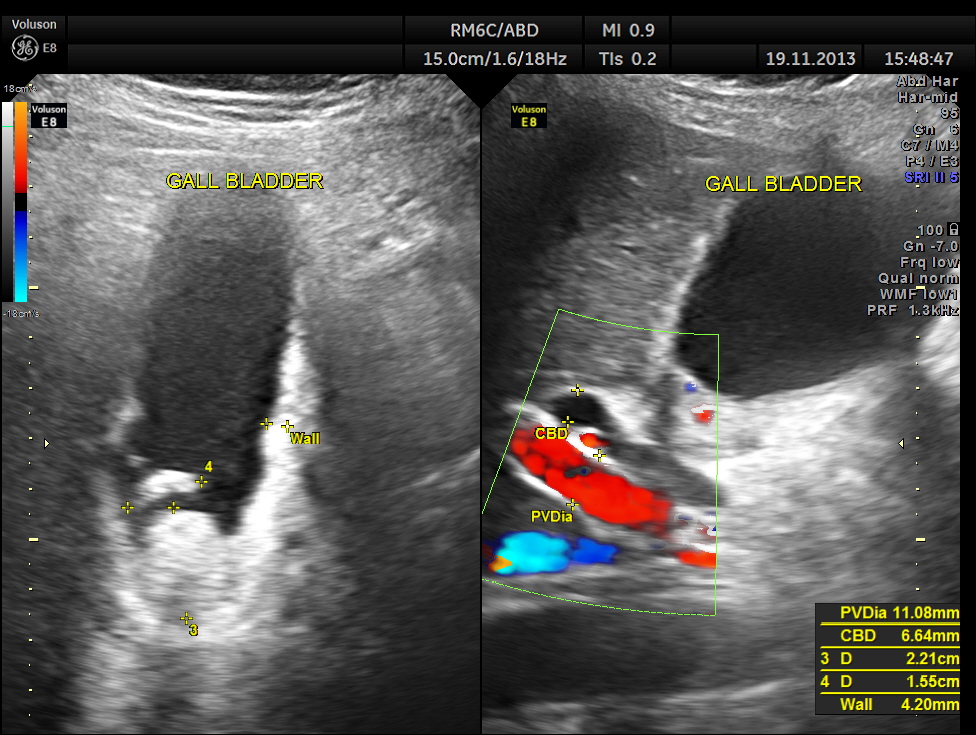
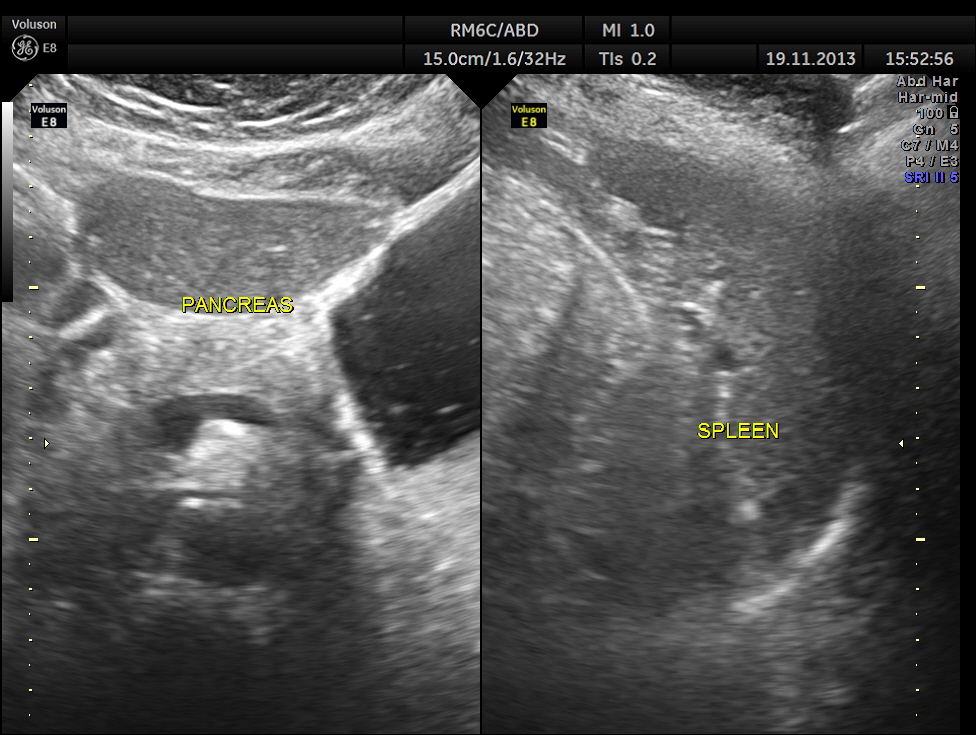
Her abdominal scan revealed a distended gall bladder with two big gallstones and one of them was obstructing the cystic duct.
She had acute cholecystitis with gallstones causing obstruction of the cystic duct.

She was referred to the surgeon and underwent laparoscopic cholecystectomy and was found to have empyema of gallbladder due to the obstruction. She had an uneventful post operative period .
This case is presented here to underline the fact that acute cholecystitis can mimic acute coronary syndrome and can have non specific T wave changes. Beware.

I think AC cholecystitis is a D.D for ACS,but for the ECG which misguided this case?There was no sign of Obst Jaundice?Thanks for reporting this interesting case,Narayanan.
LikeLike
No jaundice; but SGOT & SGPT mildly elevated.
LikeLike
Thank you for this so interesting information.
LikeLike
maravilloso
LikeLike
Learnt a very important lesson ….sir thanks
LikeLike
Thanks sir
LikeLike
Years ago I always took a routine look at the gb when doing the subcostal view for echo …i cannot tell you how many gallstones i found on patients having echo for chest pain …. then of course as medicine in the US changed I was no longer allowed to look……….. Im sure there have been thousands more
LikeLike
I can remeber a case where the opposite happened. A hospital I worked was treating a patient overnight for gallbaldder. When my co-worker and I did his ecg the next morning, he was having an acute MI
LikeLike
Sure ; we should remember that the converse can be true .thanks for the feed back
LikeLike
good debate
LikeLike
Nice case
It is classical?
ST T changes seems non specific
And we have to be a good clinician ..(history anamnesis and phisical exam!!!
Personnally systematically when i do echo cardiac i take subcostal view and i look every time the GB
We must to be clinician and echocardiographist
Nice case
Thanks
LikeLike
I agree with you
LikeLike